
Health systems, insurers, and payors have invested heavily in building digital front doors: centralized patient apps, online portals, triage chatbots, health hotlines. These are real achievements that reduce administrative friction, streamline scheduling, and improve operational efficiency. But it is worth being honest about who they primarily serve. In most cases, digital front doors have made it easier for organizations to manage patients. They have not meaningfully changed the experience of being one.
A door is only as valuable as what is behind it.
For millions of people living with chronic disease, what lies behind that front door is remarkably thin. There may be an appointment booking system, a prescription refill tool, perhaps a library of educational articles about their chronic condition, and now some kind of generic chatbot. But patients are not asking for more portals. They are asking to be heard, to have their problems listened to, real solutions offered, and support that treats them as whole people. For the person who just started a new medication for obesity, who is anxious, already inundated with “information” and is unsure where to lay their trust, the door leads to a hallway with very little in it.
The infrastructure for sustained, personalized behavioural support, the kind that actually helps people change their lives, was never built.
What behavioural support actually is, and why it matters
Behavioural support is the ongoing, structured process of helping people understand their disease and their body, adopt the changes needed to manage a chronic condition, and sustain those changes over time. It is not simply about telling people what to do. It is about helping them understand why their body responds the way it does, reframing the shame and blame that so many people living with chronic disease carry, and building the self-efficacy to manage their health with confidence. Critically, it is proactive and long term, not reactive. It prepares people for what to expect before problems arise and helps them build resilience.
Every major clinical guideline recommends it. The WHO’s first global GLP-1 guidelines call for integrated behavioural support as part of long-term obesity management. The Canadian Adult Obesity Clinical Practice Guidelines place behavioural interventions at the foundation of care. A recent joint advisory from four leading U.S. medical societies states plainly that while comprehensive lifestyle modification is recommended as part of the treatment plan for obesity, its use is not widespread in practice.
The gap between what is recommended and what is delivered is enormous. Without behavioural support, patients experience worse health outcomes, more severe side effects, and dramatically lower chances of treatment success. Fifty to seventy percent of people who need ongoing treatment for obesity stop GLP-1 medications within the first year. Much of this is preventable.
The numbers behind the gap
An analysis of NHANES data (2011–2018) found that only 40% of adults with obesity or overweight were counselled to lose weight by a healthcare provider. The ACTION study found that only 24% of patients with obesity had a follow-up appointment scheduled after an initial weight discussion. 82% considered weight loss entirely their own responsibility. Globally, the ACTION-IO study across 11 countries found a mean delay of six years between when a person first starts struggling with their weight and when they have any discussion about it with a provider. These are all lost opportunities to be able to intervene and support.
In Canada, a real-world survey published in 2025 found that for nearly 45% of patients with obesity, no healthcare professional beyond the prescribing physician was involved in their care. No dietitian. No psychologist. No behavioural support of any kind.
The prescription is written and the patient walks out the door alone.
Why this is an infrastructure problem, not a product problem
The instinct in digital health has been to solve this with products. There are now hundreds of chronic disease management apps, wellness platforms, and patient engagement tools on the market. Some are well designed and many are well intentioned. However, almost none of them work at scale for the people who need support the most.
The data is consistent: people stop using mobile apps for chronic diseases quickly. A 2024 scoping review in JMIR with over 500,000 patients found that a median of 70% of users abandoned health and lifestyle apps within the first 100 days, with diet apps reaching 86% abandonment. Well known programs like Noom, Omada, and Virta acknowledge the complexity of obesity, yet design programs that last 10, 16, or 24 weeks despite obesity being a lifelong disease. And the first question most of them ask is: how much weight do you want to lose, and how quickly? That is not treatment for metabolic disease. Rather, it is idealistic motivation that inevitably leads patients down the same pathway they have been down many times before. There is a fundamental mismatch between what wellness apps offer and what chronic disease behavioural support requires, and because wellness apps are all that exist, the two are being treated as the same thing. They are not.
There are now hundreds of chronic disease management apps, wellness platforms, and patient engagement tools on the market. Some are well designed and many are well intentioned. However, almost none of them work at scale for the people who need support the most.
The people who do use these apps tend to be younger, higher income, and already health-engaged, which is precisely the opposite of the population that needs the most support. As we wrote in a previous post on accessibility, the people who most need long-term support are the least likely to get it through traditional digital channels. This is especially true for the populations that bear the highest burden of metabolic disease: older adults, people in rural communities, and people with multiple clinical comorbidities.
The alternative is not to give up on technology. It is to choose the right channels. SMS reaches virtually every mobile phone on earth, regardless of device, income, or digital literacy. WhatsApp has over 3 billion monthly active users globally, and in many communities, particularly among Hispanic Americans, immigrant populations, and across Latin America, South Asia, and Africa, it is the primary means of daily communication. These are not niche channels – they are universal infrastructure.
Behavioural support delivered through messaging is not a downgrade from an app. It is an upgrade in reach, equity, and real-world engagement.
What nymble is building
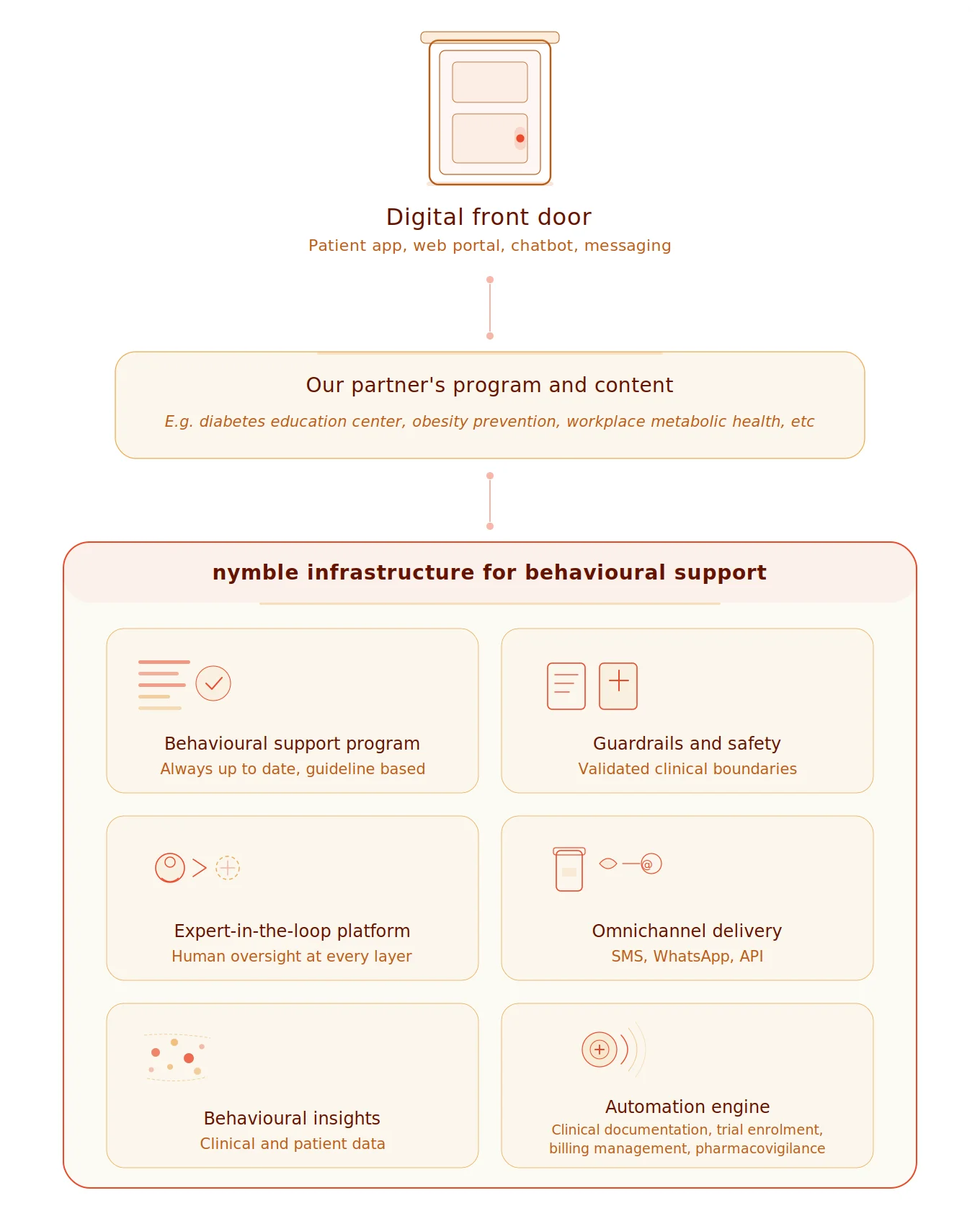
This is the work we are doing at nymble. Not building another app. Building infrastructure for behavioural support that health systems, payors, life sciences companies, and care networks can deploy into their existing environments. We are doing it alongside the clinical experts who support patients every single day, and with the joint forces of patient advocacy groups, because there is no point in building something for someone without asking them what they need.
In an era where building software is becoming commoditized, the differentiators are not code. What differentiates is a culture of agility and an infrastructure approach. nymble is purpose-built for this: structured, personalized clinical programming that helps people understand their disease and their body, reduces stigma, increases self-efficacy, and builds the capacity to manage chronic disease long term. This programming is delivered through a modular platform with clinical safety designed into the architecture, human expert-in-the-loop orchestration at every layer, and the ability to integrate through consumer messaging channels, agentic services, or API, adapting to our partner’s ecosystem rather than the other way around.
This is not a wellness app with a medical advisor listed on the about page. This is infrastructure built by the people who wrote the guidelines.
But the single factor that matters most, and the one that will increasingly matter in a world flooded with misinformation and misaligned incentives, is wide-reaching trust. nymble’s content is created and overseen by clinical experts who are not just advisors but global leaders in the field. Our co-founder and Chief Medical Officer, Dr. Megha Poddar, is a co-author of the Canadian Adult Obesity Clinical Practice Guidelines, the same guidelines now adopted and adapted in Ireland and Chile, and the global ICHOM Standard Set for Obesity. Our Clinical Advisory Board includes Dr. Arya Sharma, the former Scientific Director of the Canadian Obesity Network, Dr. Sean Wharton, one of Canada’s foremost obesity medicine specialists, and Dr. Carel Le Roux, a world-renowned researcher in the biology of obesity at University College Dublin.
This is not a wellness app with a medical advisor listed on the about page. This is infrastructure built by the people who wrote the guidelines. Rather than payors, insurers, and care networks rebuilding from scratch, nymble is a layer they can build their programs on top of. We plug into existing digital front doors and fill the hallway behind them with something that actually serves patients.
The door is open. What is behind it?
The digital front doors exist and medications are here. The patients are walking through. The question for every health system, every payor, and every organisation supporting patients in their metabolic health is: what do people find when they walk through that door?
nymble is building that support. And we are doing it alongside the partners who share our belief that people living with chronic disease deserve more than a prescription.
For organisations: learn how nymble integrates into your care pathway at nymble.health/for-organizations
For care providers: enrol your patients in nymble’s Equitable Access Program at nymble.health/for-individuals
To learn more: reach out to us at [email protected]
Dr. Puneet Seth is the founder and CEO of nymble health, a practicing family physician, and the host of the North of Patient podcast. nymble is building the most accessible and effective behavioural support platform for chronic disease worldwide.