

For three years, the dominant question in obesity care has been access: who can get a GLP-1, and who can afford one. That question is finally beginning to answer itself. In Canada, the first G7 country to reach this point, semaglutide has gone off patent and generics have arrived at a fraction of the branded cost. In the United States, Medicare has negotiated its first cuts on drug prices (a roughly seventy percent cut taking Ozempic from about $959 a month toward $274), alongside deals that put marketed injectables near $245 for Medicare and Medicaid and extend obesity coverage to Medicare for the first time. Across other markets the same pull is taking hold as patents lapse and payers push back on price. The molecule, for so long the bottleneck, is becoming abundant and affordable.
This is good news, and worth celebrating. But falling prices and widening coverage expose something we were able to ignore while the drugs were scarce and expensive: once the molecule is in someone’s hands, we have built almost nothing to help them succeed with it. And this is not really unique to obesity. It is the pattern across chronic disease, in diabetes, inflammatory bowel disease, asthma, nearly every chronic disease I’ve seen as a family doctor: we prescribe, then leave people to do the hardest part, dealing with how their life needs to accommodate this new condition, largely on their own. Obesity simply makes it impossible to ignore, because it is a new frontier of treatment for a condition only recently recognized as a disease, with almost no infrastructure behind it.
The term “miracle drug” is too often thrown around with GLP-1s, and some of it is true – these medications are incredibly safe and effective. Yet a miracle handed over at the counter is not the same as care. We found a way to effectively treat the biology so that people could better engage in behaviour change, and then left them hanging. Somewhere in the rush to make the molecule cheaper and easier to get, we let ourselves believe that the prescription was the finish line. It was always the starting line: the beginning of a long, largely unsupported walk that we ask people to take by themselves.
The months that no one owns
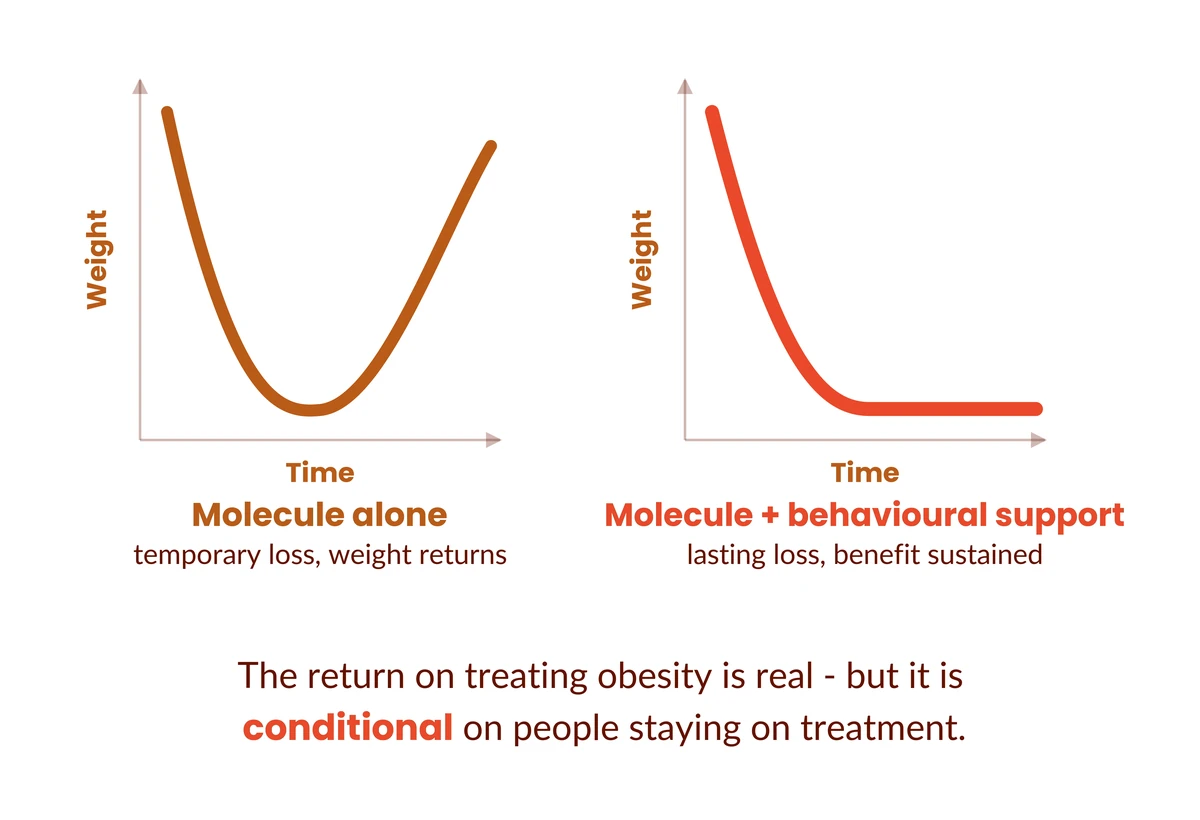
Consider what actually happens after the prescription. Imagine someone four months into treatment. The medication is working exactly as designed. Their appetite and food noise was magically suppressed to the point where it felt like a miracle, but as their weight decreased and their appetite hormone continued to increase, their appetite centres in their brain started to increase the desire to eat. Nobody prepared them for this. They read the silence not as the drug succeeding but as something being wrong, and they stop. Three months later the weight is back and so is their cardiometabolic risk. The molecule did everything we asked of it; the support that would have carried them through that moment simply did not exist.
We found a way to effectively treat the biology so that people could better engage in behaviour change, and then left them hanging.
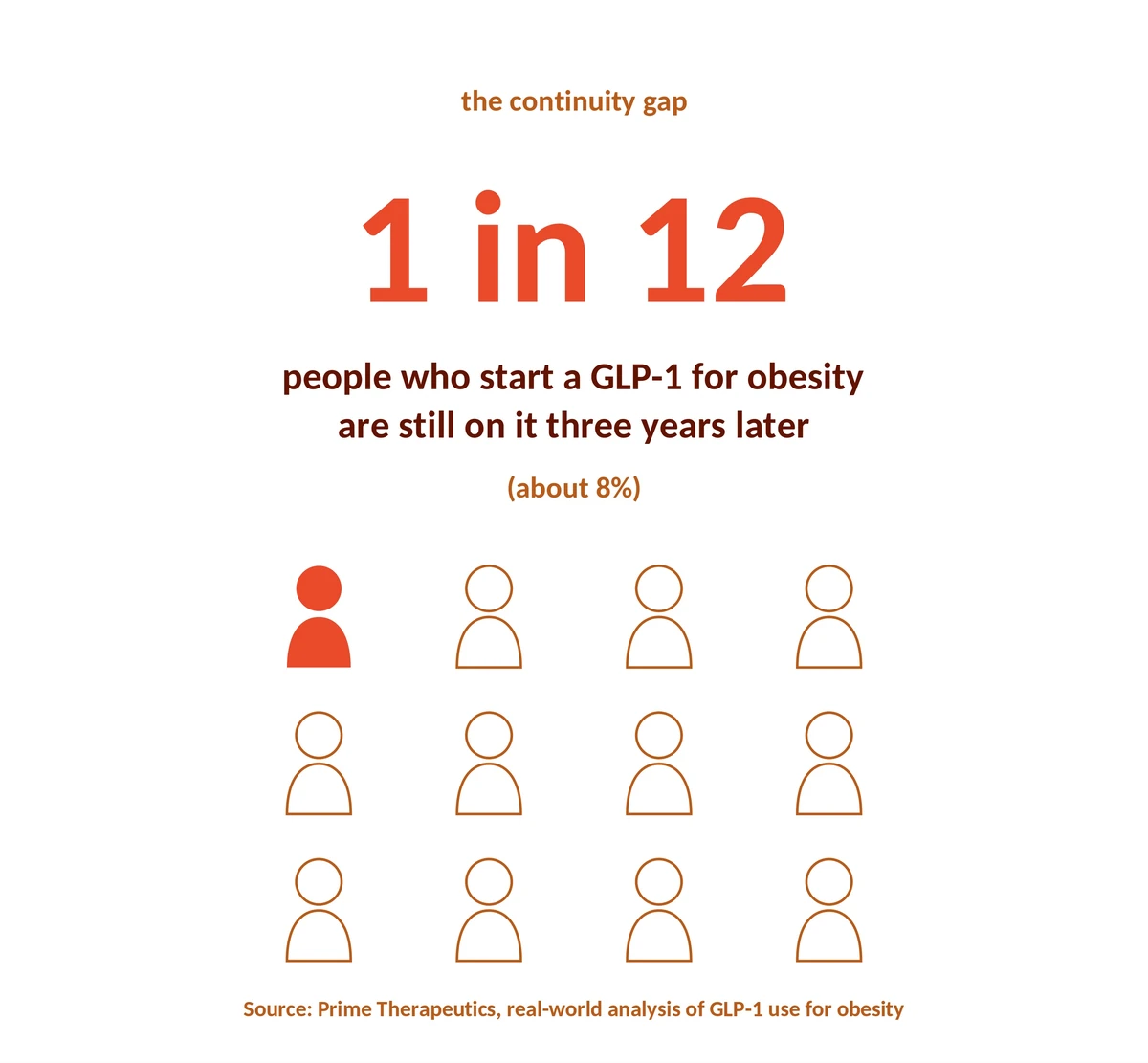
This is not a rare story. It is closer to the typical one. The most rigorous real-world data we have, from Prime Therapeutics, found that only 1 in 12 people who started a GLP-1 for obesity were still taking it three years later, about eight percent. Even for the newest and most effective medications, it was about one in seven. We are prescribing a lifelong treatment for a lifelong disease and losing most people within the first two years, and we have organised ourselves, almost perfectly, to think that we need to focus on improvements in drug development as opposed to facing the real problem.
Much of that loss of health gain is preventable, and almost none of it is the patient’s or the drug’s fault. The reflex in digital health has been to close the gap with products. I have written before about the empty hallway behind the digital front door. Health systems built the portals, the apps, and the chatbots, but never built what patients actually walk in looking for. The data is unforgiving: a 2024 review of more than half a million users found a median of seventy percent abandoned health and lifestyle apps within a hundred days, with diet apps reaching eighty-six percent. And those who do stick tend to be younger, higher-income, and already healthy, the opposite of the population carrying the heaviest burden of disease. Strip it down and the problem is simple: the hard work of behavioural change has only ever had two delivery systems, and neither scales. Skilled people, who cannot be everywhere at once, and one-off apps, which most people abandon. In both scenarios, the patient inevitably ends up blaming themselves.
We are measuring the wrong thing
Part of the reason we miss all of this is that we are measuring the wrong things. We track milligrams and pounds and almost never capture the behavioural, experiential signal that actually predicts who will do well. Closing that gap is the part of this story I think the field most underestimates. A patient who gains two pounds but tells me, for the first time, that she has stopped blaming herself and begun to understand her own biology is a patient who is going to do well over the long term, and there is no box on any form to record it. We celebrate the number on the scale and stay blind to the thing underneath it that decides whether the number lasts.
A prescription is a promise, not an outcome.
There is a deeper assumption worth questioning, too. Lifelong therapy is the right default on today’s evidence, but it is already evolving. Part of why we prescribe indefinitely is that we still treat obesity as one monolithic condition, and it almost certainly is not. People reach the same diagnosis by very different biological and behavioural routes, and that biology can persist: Hinte and colleagues found that fat cells retain an epigenetic “memory” of obesity long after weight loss, one that may prime the body to regain rather than reflect any failure of willpower. The clinical picture mirrors this: when treatment stops, much of the weight and metabolic benefit comes back. But that is the case for sustained support, not against it. The future is not “everyone on the same molecule forever”; it is precision care, knowing who can step down, who should stay the course, and who needs more support rather than more medication. None of which is possible without the one thing we keep discarding: the patient’s lived experience.
What this moment in AI is really telling us
It would be easy to assume artificial intelligence closes this gap on its own. I am an optimist about AI in medicine, but I want to be clear-eyed about what it is doing right now, and what it is not. AI has made software and health “content” nearly free, which is exactly why every feed is now full of it, and why the one thing chronic-disease care cannot function without, trust, is getting harder to find rather than easier. When anything can be generated, the scarce asset is no longer information. It is a relationship a person genuinely believes in, grounded in real clinical authority, that shows up over months and years and helps them change. AI does not manufacture that. Used well, it can extend it to far more people than any clinic ever could.
The most expensive version of the story
This is the moment for the organisations that pay for and deliver care (insurers, health systems, networks, employers) to decide what kind of investment they are actually making. As the molecule gets cheaper, the easy move is to treat the lower price as the win and stop there. Peter Singer has modelled the economic return of treating obesity properly, and the return is real. But, as he is careful to note, it is conditional on people staying in treatment over the long term. That condition is the whole game.
Paying for the molecule while leaving continuity unfunded is not a saving; it is the most expensive version of this story: the one where we underwrite temporary weight loss and forgo the lasting benefit, for the person and for the system alike. The organisations that look prescient in five years will be the ones building the support layer now, rather than discovering its absence in their claims data later.
What we’ve built
This is the work we are doing at nymble, and why we have been deliberate about not building “another app.” We have built the infrastructure for behavioural support, the part that belongs behind the digital front door that has never been built, starting in obesity, and extending to the chronic diseases that share the same gap. It reaches people where they already are, through ordinary text and WhatsApp rather than another download, because the people who most need continuity are the least likely to get it through a high-friction app.
What gives me confidence is the foundation: clinical programming overseen by the authors of the obesity guidelines themselves, and the nymble score, our way of capturing the lived experience the system discards so that support can adapt to each person.
These medications are the most important thing to happen to this field in a generation. But a prescription is a promise, not an outcome, and right now we are breaking that promise in the long, quiet months after the patient leaves the room. The work that remains is not more molecules, and not more apps. It is the unglamorous, human work of helping people stay the course, and of building the infrastructure that makes that support as dependable as the prescription itself. To the insurers, systems, and partners who can see that the next chapter is not about the drug but about everything that surrounds it: the prescription was never the finish line. What comes after it is no longer missing. We have built it. The work now is to put it in the hands of the people who need it, with you.
If you’re working on this problem, from inside a health system, a payor, a research group or other stakeholder, we’d love to hear from you. Contact us at [email protected].
If you are a patient looking for support on your weight management journey, find out more here.
Dr. Puneet Seth is Co-founder and CEO of nymble health, a practicing family physician in Canada, and a serial digital health entrepreneur. nymble is building infrastructure for accessible and effective behavioural support for chronic diseases such as obesity.